The WHO ICD-11 classification is very different from the 10th version that the United States modified to create the ICD-10-CM code set that is used for reporting healthcare services on claims in the US today. One distinct difference is ICD-11 codes can be either pre-coordinated or post-coordinated, whereas all ICD-10-CM codes are post-coordinated.
Let’s compare codes for a common condition, atherosclerotic heart disease, to illustrate this difference.
Note:
- These code assignments reflect the closest equivalent code from each code set as of May 2023.
- Code category comparisons reflect excerpts from the ICD-11 Browser compared to segments from the ICD-10-CM Tabular listing.
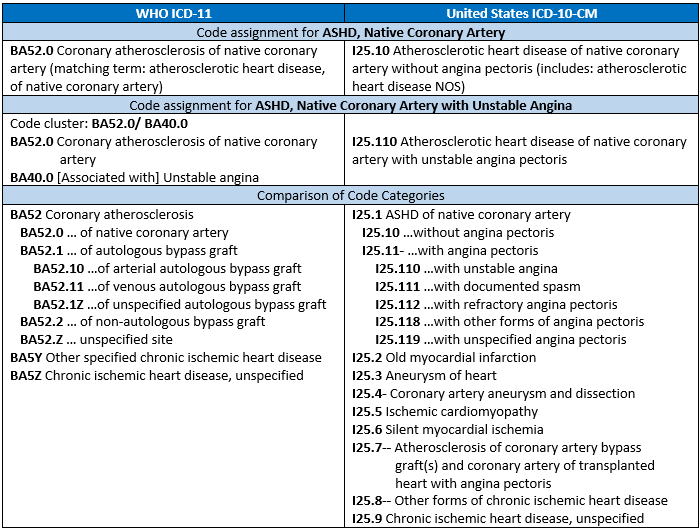
The examples in the table above illustrate both pre-coordinated and post-coordinated codes in ICD-11 for atherosclerotic heart disease (ASHD). The first example is a pre-coordinated ICD-11 code that reflects both the ASHD and that it is of the native coronary artery (BA52.0). In the second example, a post-coordinated ICD-11 code cluster reflects both the ASHD of native coronary artery and the unstable angina associated with the ASHD.
Guidelines within the ICD-11 code set, called “sanctioning rules,” provide guidance for pre- and post-coordination. ICD-11 presents multiple post-coordination code options for coronary atherosclerosis including specific anatomy (e.g., XA0F62, left main coronary artery), manifestations (e.g., BD10, congestive heart failure), associated conditions (e.g., BA41, acute myocardial infarction), and severity (e.g., XS8U, multiple vessel disease). As with ICD-10-CM today, clinical documentation must specify post-coordination codes are associated with the main condition to link them in a code cluster.
Go to the WHO ICD-11 homepage to browse ICD-11 codes and review the various post-coordination details. You can also review the WHO’s ICD-11 Reference Guide for ICD-11 coding conventions and guidelines.
Mary H. Stanfill is Vice President of Consulting for United Audit Systems, Inc. and is the official representative of the IFHIMA to the WHO Family of International Classifications Education and Implementation (EIC) and Morbidity Reference Group (MbRG) workgroups. She has over 35 years of experience in the health information profession, primarily focused on clinical classification of healthcare data. She holds a masters in biomedical informatics and is currently pursuing a doctorate in health informatics.
Email: mstanfill@uasisolutions.com