
Medical Coding Examples & Tips for Everyday Coding Success
Explore concise, expert-driven medical billing and coding examples that
breaks down complex scenarios into
clear, usable insight.
Just released: The 2026 HCC Passport
Updated for 2026, this practical resource supports coders and healthcare leaders with defensible HCC documentation and coding guidance to improve compliance, reduce risk, and impact RAF outcomes.
2026 ICD-10 Coding Tip Guidebook Now Available!
Stay Current and Enhance Accuracy with UASI’s Professional Guidance
Get instant access!
Coding Tips
Welcome to UASI's Coding Corner! We're here to make your medical coding journey smoother and more enjoyable with our friendly and practical tips. Whether you're just starting out or you've been in the field for years, you'll find something useful here. Our expert advice, handy tricks, and up-to-date industry insights are all geared towards helping you code more accurately and efficiently. So, grab a cup of coffee, get comfy, and explore our tips to take your coding skills to the next level!

Review ICD-10-CM pregnancy coding guidelines, including Chapter 15 codes, trimester selection, and weeks of gestation coding.
Learn the new ICD-10-CM codes for thyroid eye disease (TED), including H05.831–H05.839, with coding examples and documentation guidance.
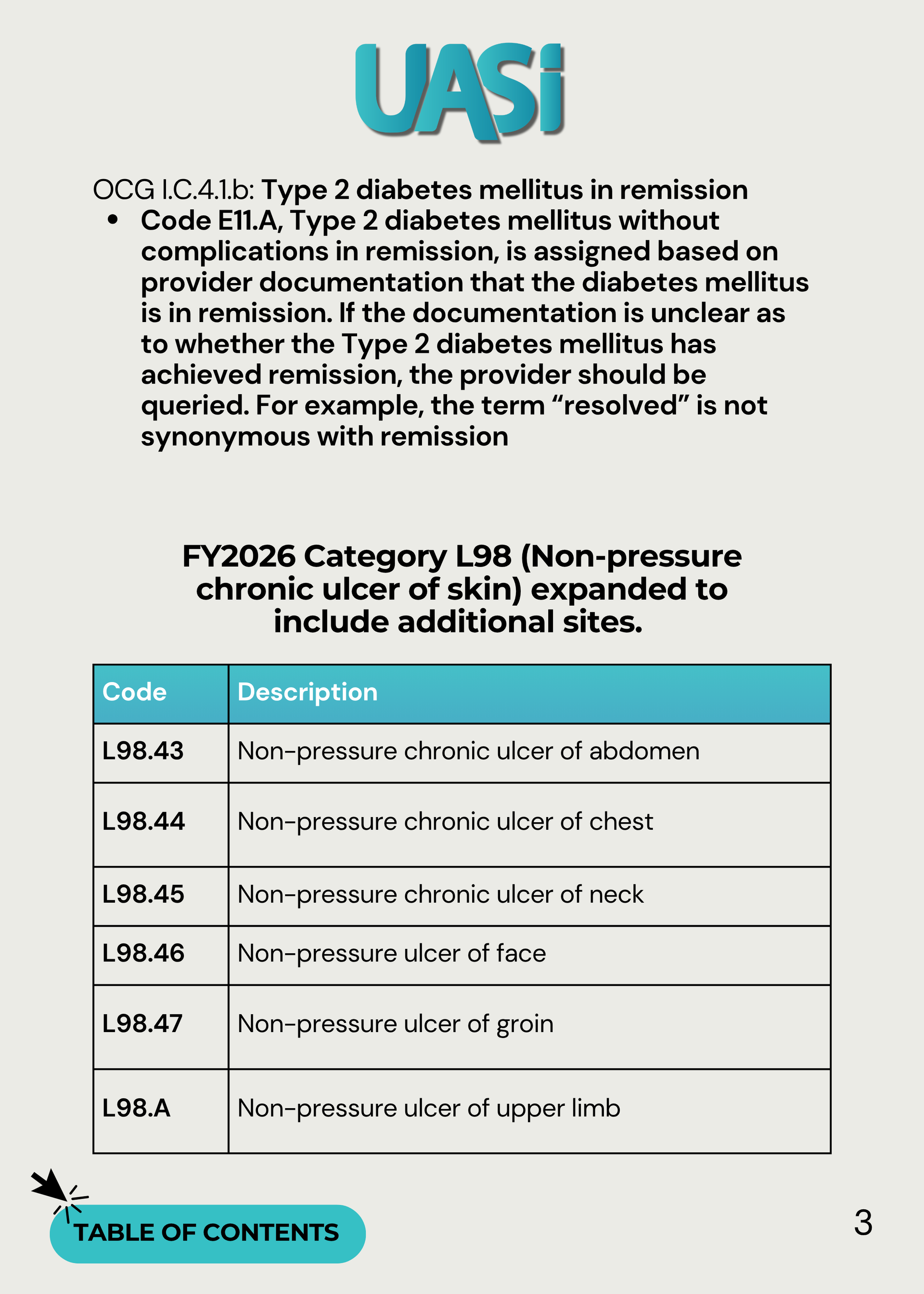
Learn when to assign E78.0 for hypercholesterolemia in ICD-10-CM, including coding rules, distinctions from hyperlipidemia, and common pitfalls.
Learn how to code encephalopathy in ICD-10-CM, including types, documentation tips, query opportunities, and FY 2026 coding guidance.
Learn how to code MASLD and MASH using ICD-10-CM terminology, including NAFLD and NASH equivalents, documentation tips, and coding guidance.
Learn ICD-10-PCS coding for AAOLCA transconal unroofing procedures, including Release and Supplement root operations, documentation tips, and coding guidance.

Learn how to code paclitaxel-coated balloon use during PCI, including ICD-10-PCS New Technology codes, documentation requirements, and sequencing guidance.
Understand how to report Fontan-associated conditions using ICD-10-CM category I27.84. Learn documentation considerations and coding guidance for complications of Fontan physiology.
Understand cerebral edema ICD-10-CM coding, including traumatic vs. non-traumatic distinctions, associated codes, documentation requirements, and treatment considerations.

Clarify ICD-10-PCS coding for the PillSense ingestible capsule used to detect upper GI bleeding, including documentation requirements and new technology code XDJ07LB.
New prostate biopsy CPT codes effective January 1, 2026, including lesion-based reporting, bundled imaging, and documentation requirements for accurate coding.
Clarify how to code fibrin sheath disruption during dialysis catheter procedures, including venous angioplasty guidance and Coding Clinic direction.

Identify Sandifer syndrome documentation requirements and ICD-10-CM coding guidance, including GERD sequencing and associated neuromuscular manifestations.

Learn about the difference between adverse effects and poisoning in ICD-10-CM. Learn sequencing rules, examples, and documentation tips for accurate T36–T50 coding.
Understand when radiology can support ischemic stroke (CVA) coding specificity without inferring mechanism. This UASI coding tip reviews Coding Clinic guidance, examples, NIHSS reporting, and query best practices.

When can possible, probable, or suspected diagnoses be coded? This coding tip explains inpatient vs outpatient rules, discharge summary requirements, and when a query is required.
Stay ahead with UASI's
Monthly Coding Tips
Featuring practical advice, industry updates, and best practices to enhance your coding accuracy and efficiency. Sign up below to receive monthly coding tips directly to your inbox!



{kind=link}
{kind=link}
{kind=link}